Bodybuilding can be a demanding physical activity that places stress on various parts of the body, including the joints. Knee pain is a common issue that some bodybuilders may experience. Several factors can contribute to knee pain, and it’s essential to address them to prevent further discomfort and potential injury. Here are some considerations:
- Improper Form: Poor form during exercises like squats, lunges, or leg presses can put excessive stress on the knees. Ensure that you have proper technique and consider working with a qualified personal trainer to perfect your form.
- Overtraining: Overtraining, or excessive training without adequate rest, can lead to overuse injuries, including knee pain. Make sure you have a well-structured training program that allows for sufficient rest and recovery.
- Inadequate Warm-Up and Stretching: Skipping warm-up exercises and not stretching properly before lifting weights can increase the risk of injury. Proper warm-up and stretching can help prepare your muscles and joints for the workout.
- Muscular Imbalances: Muscle imbalances in the lower body, particularly in the quadriceps and hamstrings, can affect knee stability. Incorporate exercises that target both muscle groups to maintain balance.

- Footwear: Wearing the wrong type of footwear, or shoes that lack proper cushioning and support, can contribute to knee pain. Invest in good-quality, supportive shoes for your workouts.
- Nutrition and Hydration: Proper nutrition and hydration are essential for overall joint health. Make sure you’re getting enough nutrients to support joint function, such as vitamins and minerals like calcium and vitamin D.
- Avoiding Overloading: Gradually increase the intensity of your workouts and the amount of weight you lift. Overloading your body too quickly can lead to injuries.
Incorporating exercises that strengthen the muscles around the knee, such as the quadriceps, hamstrings, and calf muscles, can also help provide stability and support to the knee joint. Additionally, using proper equipment like knee sleeves or braces, when necessary and advised by a healthcare professional, can provide extra support.
If you’re experiencing chronic or severe knee pain, it’s crucial to consult with a healthcare professional or physical therapist for a proper evaluation and personalized recommendations. They can help determine the underlying cause of your knee pain and develop a treatment plan tailored to your needs.
How the Knee Joint Works
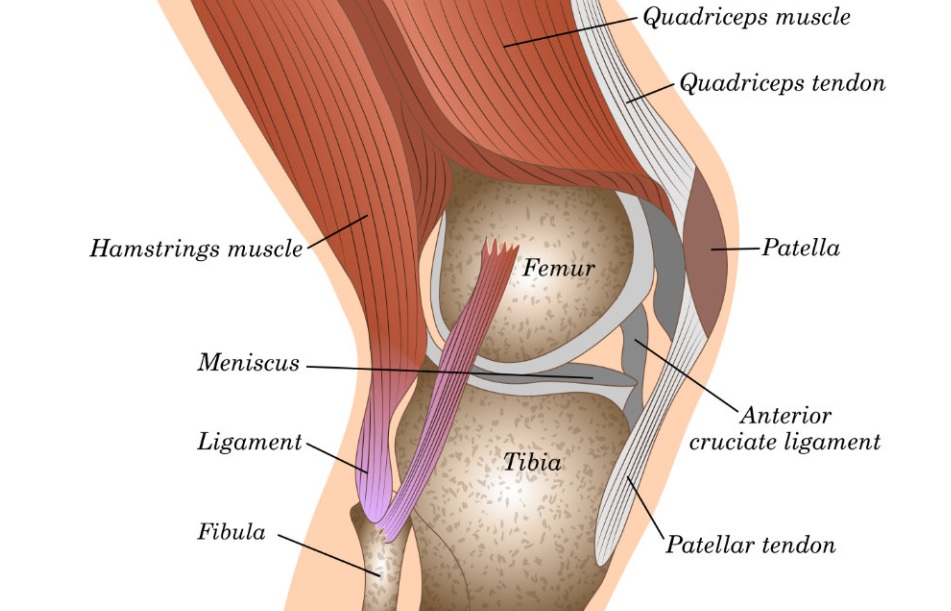
Knee movement is a complex process that involves the coordinated interaction of bones, ligaments, muscles, tendons, and other structures. It allows for various types of motion, primarily flexion (bending) and extension (straightening), as well as a small degree of rotation. Here’s how knee movement works:
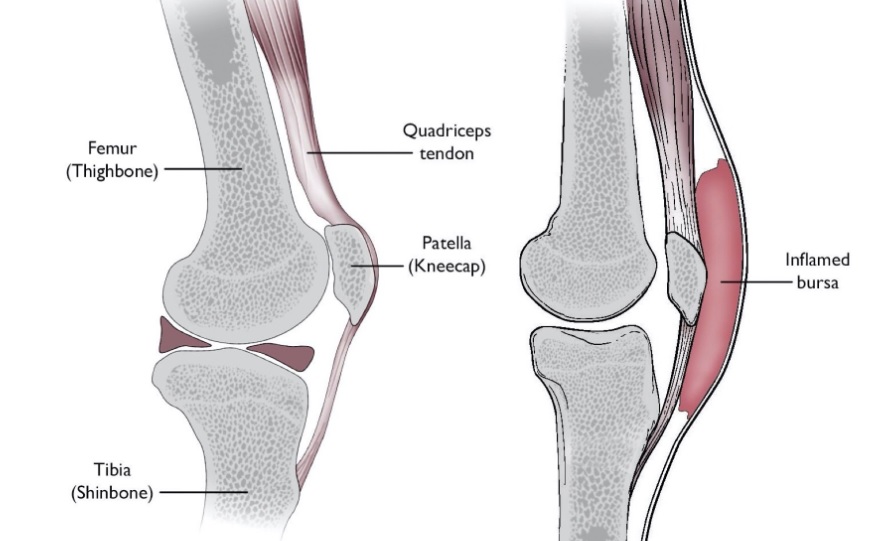
- Bones: The knee joint involves three bones: the femur (thigh bone), tibia (shinbone), and patella (kneecap). These bones articulate with each other to form the knee joint.
- Articular Cartilage: The ends of the femur, tibia, and patella are covered with articular cartilage, which is a smooth, slippery tissue. This cartilage serves as a cushion and allows the bones to glide smoothly against each other during movement.
- Meniscus: Inside the knee joint are two C-shaped cartilaginous structures called the medial and lateral menisci. These act as shock absorbers, provide stability, and help distribute the load within the joint during movement.
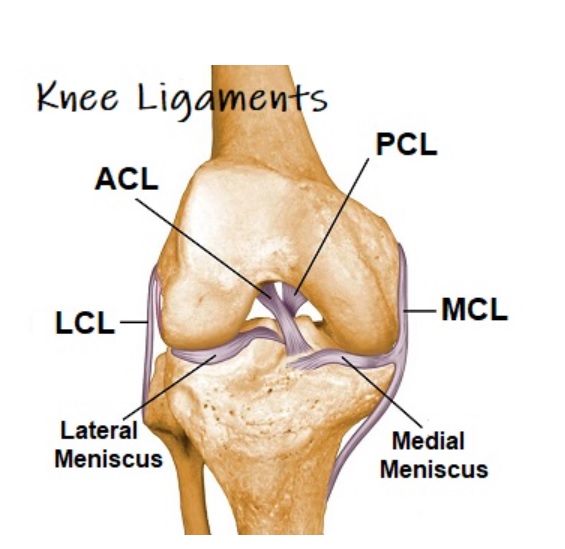
Ligaments: The knee joint is stabilized by several ligaments:
- Anterior Cruciate Ligament (ACL): Prevents the tibia from moving too far forward relative to the femur.
- Posterior Cruciate Ligament (PCL): Prevents the tibia from moving too far backward relative to the femur.
- Medial Collateral Ligament (MCL): Provides stability against inward (valgus) forces.
- Lateral Collateral Ligament (LCL): Provides stability against outward (varus) forces.
- Muscles: Muscles around the knee play a crucial role in knee movement. Two muscle groups are particularly important: Quadriceps are located on the front of the thigh, and these muscles are responsible for knee extension (straightening) while Hamstrings are located on the back of the thigh and are important for knee flexion (bending).
- Tendons: Tendons connect muscles to bones and transmit the force generated by muscles to the bones they move. For example, the patellar tendon connects the quadriceps muscles to the tibia and is involved in knee extension.
- Synovial Membrane and Synovial Fluid: The synovial membrane lines the inner surface of the joint capsule and produces synovial fluid. This fluid lubricates the joint, nourishes the articular cartilage, and reduces friction during movement.
Knee Movement Occurs Through the Following Actions:
- Flexion: Bending the knee, bringing the lower leg closer to the thigh. This action is primarily initiated by the hamstring muscles contracting and pulling the lower leg toward the thigh.
- Extension: Straightening the knee, returning it to a fully extended position. This action is primarily driven by the quadriceps muscles contracting to pull the lower leg away from the thigh.
- Rotation: The knee joint allows for a limited degree of rotation, primarily in a seated or crossed-legged position. However, the primary function of the knee is flexion and extension rather than rotation.
The coordinated contraction and relaxation of muscles, along with the stability provided by ligaments, allow for controlled and precise knee movement. This complex interplay of structures enables us to walk, run, jump, squat, and perform a wide range of activities that require the use of our lower limbs.
Some of the Common Knee Issues
Knee pain can manifest in various forms when engaging in bodybuilding exercises. Here are some common forms of knee pain that bodybuilders may experience along with the exercises that could trigger them:
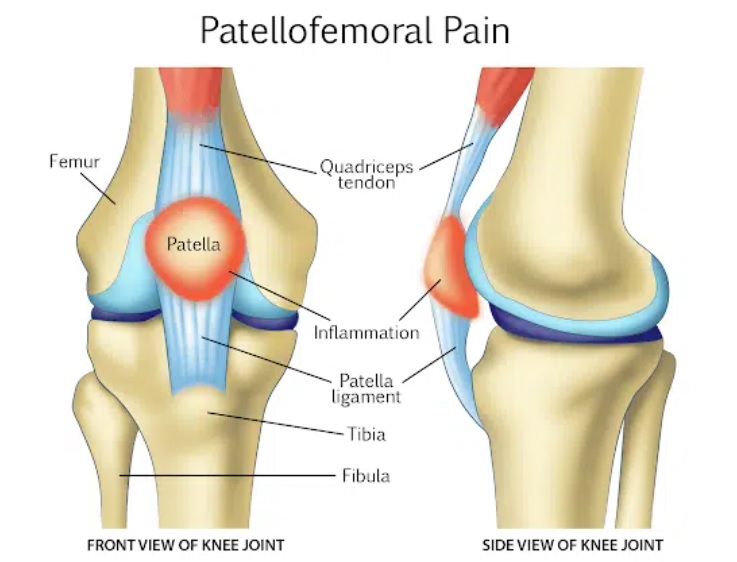
- Patellofemoral Pain Syndrome (PFPS): Also known as “runner’s knee,” PFPS involves pain around or behind the kneecap (patella). Triggering Exercises include squats, lunges, leg presses, and other exercises that involve repetitive bending of the knee.
- Iliotibial Band Syndrome (ITBS): ITBS is characterized by pain on the outer side of the knee joint. It can be triggered by leg presses, lunges, and squats can contribute to ITBS when performed with poor form or excessive volume.
- Meniscus Injuries: Tears or damage to the meniscus, the cartilage in the knee joint, can result in sharp or locking pain. Deep squats and exercises that involve twisting or pivoting motions can increase the risk of meniscus injuries.
- Anterior Cruciate Ligament (ACL) Sprains or Tears: ACL injuries often result in sudden, severe pain and instability in the knee. Exercises involving quick changes in direction, such as plyometrics or sports-specific drills, can increase the risk of ACL injuries.
- Medial Collateral Ligament (MCL) Sprains or Tears: MCL injuries may cause pain and swelling on the inner side of the knee. Movements that involve excessive force on the inner knee, such as heavy leg presses with poor form, can lead to MCL injuries.
- Tendonitis: It can cause pain and inflammation in the tendons around the knee, such as patellar tendonitis (jumper’s knee). Exercises that involve repetitive jumping, like box jumps or plyometrics, can contribute to patellar tendonitis.
- Bursitis: Bursitis involves inflammation of the bursae, small fluid-filled sacs that cushion the knee joint. Lunges, squats, or kneeling exercises that put pressure on the knee can lead to bursitis.
Fixing Your Knee Issues
The common causes of knee pain are usually because of mobility, biomechanical/muscular imbalance or load tolerance. If you feel the pain that comes on with certain exercises, or as the load increases, well, this usually is good news. If you can trace the symptoms back to the source, then they can also be corrected.
- If you experience knee pain laterally, that’s because of the iliotibal band and the quad is pulling your kneecap out of position. But, if you feel the pain on the inside or lower part of the kneecap, this is the medial patellar ligament which could be because of hip or ankle mobility issues.
- Press your kneecap in every direction so it moves comfortably from side to side. If you experience tenderness in the inferior part, below the kneecap or down where the patella attaches to your shin – well, this could be an indication of knee tendonitis.
- First, take off your shoes and do an air squat. If one of the feet starts to turn out after a few reps, this is not a good sign. And, if you cannot squat down your hamstrings and calves – also not a good indication.
- Let’s now do a single leg squat on both sides for rep. Squat down as low as possible paying attention to your knee – if you notice drifts towards your midline or shaking violently – it’s an indication or problem.
- One of the root causes of all problems is usually hip and ankle mobility issues. With one foot on the ground, take your knee and bring it to your chest. Well, if you can’t do this, then again, that’s because there’s an issue.
- Now, test your internal and external rotation of the hip. Lie on your back, put your knee at 90 degrees and then bring your foot towards the midline. To test internal rotation, you can do the exact opposite. Around 40 to 60 degrees is considered a good range for external rotation and 30 – 45 degrees for internal rotation – and if you are having a problem reaching either, then this actually could be one of the reasons.
- Testing your ankles: We need to test both sides individually. Face the wall, set that foot up five inches away from the wall and when you are about a third of the way while keeping your heel glued to the floor, drive your knee forward – and if you cannot touch the wall – well, we have found your ankle issue.
- Testing your Squat: Shoes off, feet flat on the ground and lift your toes high as they go – if you are facing a problem with your toes going off the ground, this could be because your tibialis anterior is not strong enough to dorsiflex the feet.
Step Two: Corrective Movements to Resolve Knee Pain
- Let’s look at the test where you couldn’t move the knee to your chest as you laid back: You need a foam roller and a resistance band. You can wrap that band around your ankle and scoop back till there’s tension on the band. Place that foam roller underneath your Achilles and lay your back. You need to let that tension relax your hip down to your ankle joint. Hold for two rounds on each side.
- Internal rotation problem: Line your back, bend your knees and take the foot on the side you want to work first. Step it out six inches, take the opposite leg, put it over the top and apply force. Try to drive that medialis towards the floor – hold it for 30 to 60 seconds and do a few rounds. If you feel pinching, it could mean your hip joint is impinged – add traction with a band from the side, this should sort the problem.
- For external rotation issues: Find out where the issue is most prevalent. Lunge forward, drive that knee out, twist it away from it, twist it towards it and then change the angle of the knee – do it like reps, dive into a few seconds, dive out – keep it going till it relaxes. You can go on to another variation and keep going till it’s completely cleaned up.
- Restriction issue in your ankle joint: Get a tennis ball and position it in the gap in front of your ankle bone – apply pressure to that ankle bone and drive it back releasing any built-up issue. Flex your toes away and towards your shin to work around the ball, do the same thing on the opposite side by pressing down with your hand and you should feel the relief in the ankles.
- Calves: Another issue that may be causing your knee problem could be your calves. Throw some smaller weight on the bar, cross your legs, lift your back up and then roll back and forth till that calf is released. Don’t roll out on the Achilles as it can inflame and make your ankle problem even worse.
- Still feeling that knee pain: Your medials and lateralis can cause microdysfunction as they might be pulling in opposing directions based on fiber orientation – if there’s tightness and weakness in your ad or abductors, it can cause the knee to be affected sideways.
- How to fix this: Two variations of split squats. Wrap a band around your knee, now do the exact opposite, you will be doing a lot of reps and sets and you’r not going to get to the point of having to add weight, as your problem might just be fixed.
- The dorsiflexor muscles, your tibialis anterior, your extensor digitorum longus – you need to do two things, first, do a deep squat every day. One foot at a time, contract those muscles, not just shift your weight from side to side, but actual contraction itself causes you to shift – as you will be targeting the exact muscles to get that knee into a proper alignment during a squat.
- Training your anterior tibs: Turn your toes in and out for a few sets. Work on increasing load tolerance – Spanish squat is a better option as you are in complete control of how much pressure you take off your knees, it’s all about proper positioning, maintaining good form, engaging your abductors, glutes and the anterior tips.
- Isometric version: Wrap that band around the back of your knees, and walk back till there’s enough tension to maintain good form. Drop down to 45 degrees, and hold for 60 seconds for three rounds – isometric holds help you decrease pain and reduce cortical inhibition. The key to increasing load tolerance is to find a movement you can do pain-free and then slow down to allow the muscles and tendons to do their job. You can start doing Spanish squats for reps.
- The stair-stepping method: You can do 10 degrees, to a 15 after a certain point, then start adding weight. Through the entire process of load tolerance, make sure you check in with yourself and see you are ready to move to the next step.
- Isometric hold: You can do it for reps, either add weight or move to a decline board, increase the angle to the point where you can’t anymore and add weight, by that point your knees will be solid.